Antibody positive disease
Antibodies to citrullinated protein antigens (ACPA) and rheumatoid factor (RF) and the effect they have on RA
What is seropositive RA?
Rheumatoid arthritis is a systemic autoimmune disease that mainly affects the synovium, causing progressive, symmetric, erosive destruction of cartilage and bone.1 It can be divided into two major subsets differentiated by the presence versus the absence of autoantibodies, namely antibodies to citrullinated protein antigens (ACPA) and rheumatoid factor (RF).2 Antibody positive disease is known as seropositive rheumatoid arthritis and accounts for approximately two thirds of all presentations.2
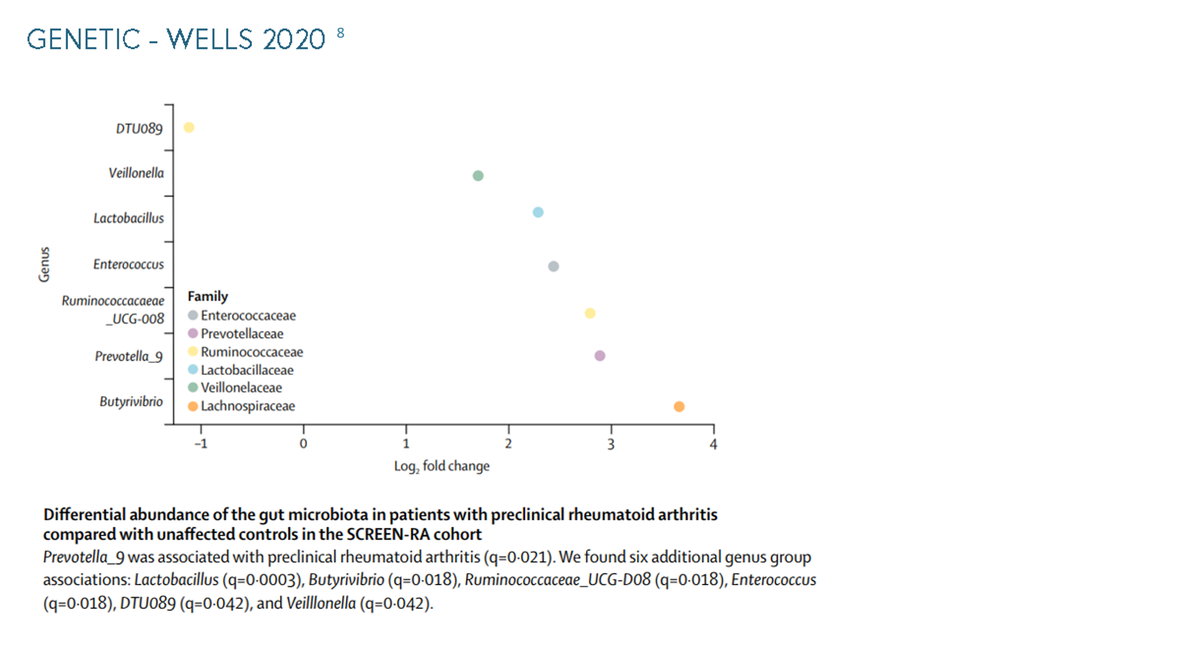
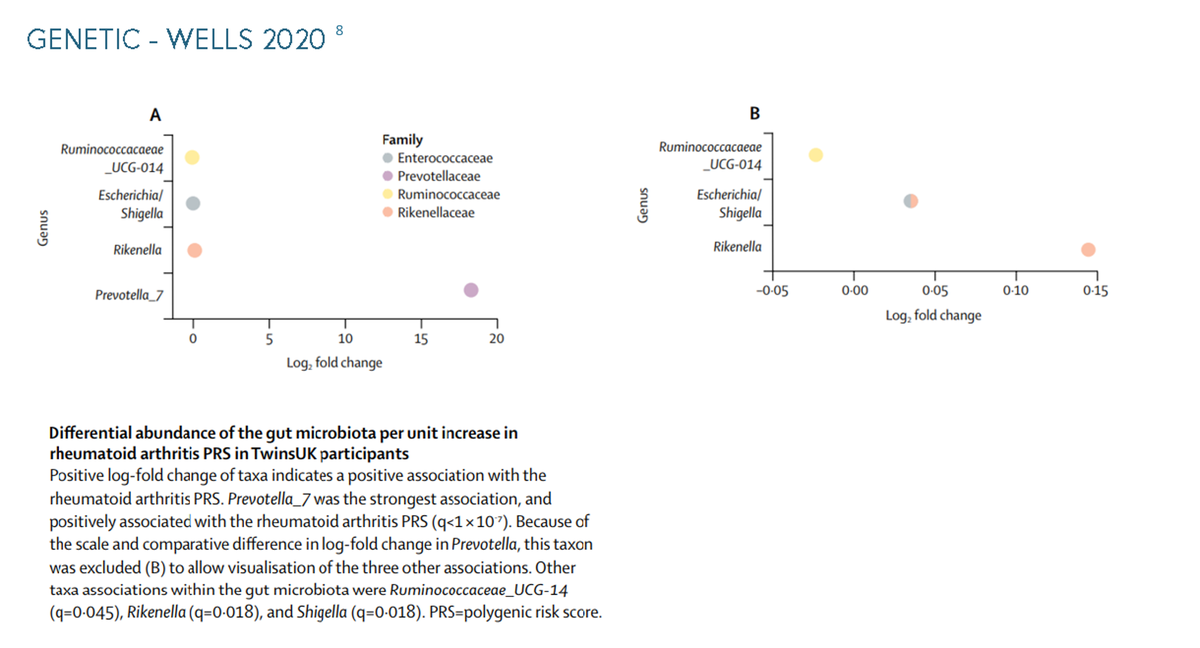
Susceptibility to autoimmune diseases is affected by both genetic and environmental factors.3 In rheumatoid arthritis, the shared epitope (SE) plays a critical role as a genetic risk factor and often results in highly aggressive, erosive disease.4 5 6 7 The difference in abundance of gut microbiota has a direct effect on rheumatoid arthritis, in a study with 172 microbial taxa present in the gut of more than 5% of participants, Prevotella_7 has the strongest taxon associated with the polygenic risk score of rheumatoid arthritis.8 Environmental factors that can affect the susceptibility to autoimmune diseases can include air pollution, gender and obesity.9 More examples of environmental factors can be seen in the information below, along with supporting graphs for the genetic factors. To see more graphs please click through.
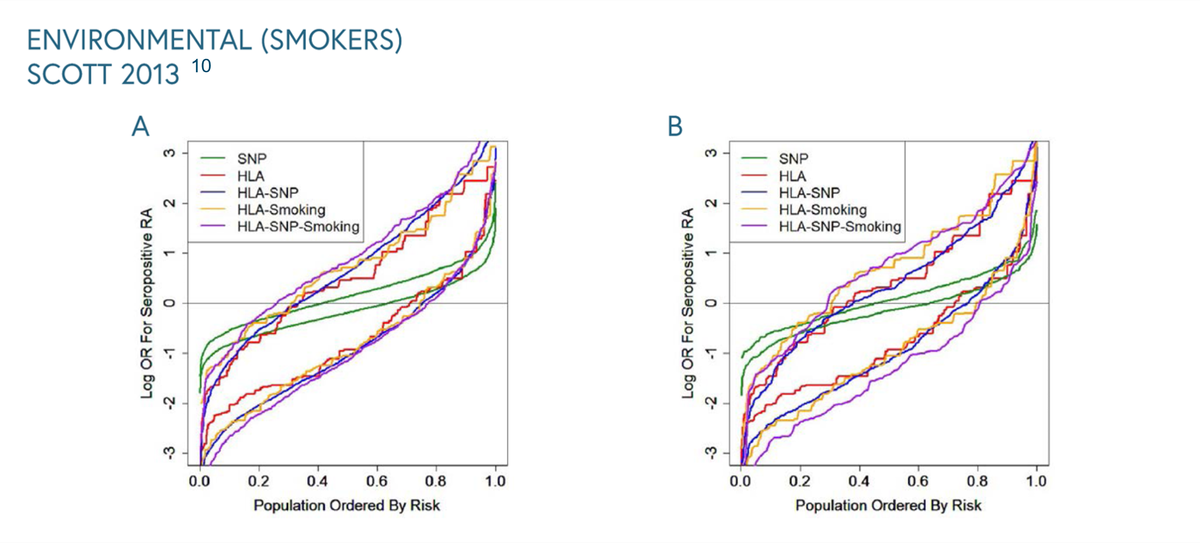
The relationship between smoking and genetics can be seen in the graph below from a study from 2013. In both datasets, the HLA model provided most risk prediction generating substantially higher and lower ORs for RA in cases and controls respectively compared with the SNP model.10 To see more graphs please click through.
Certain mutations in the human leukocyte antigen (HLA) gene predispose the immune system to more readily bind citrullinated self-proteins and recognise them as foreign, resulting in the formation of pathogenic autoantibodies against those proteins.5 6 7

Why is it important?
Seropositivity for both ACPA and RF can amplify the proinflammatory macrophage response, resulting in accelerated disease.11 12
The risk conferred by the SE is increased in a multiplicative way by exposure to various environmental pollutants, such as cigarette smoke.3 Lifestyle modifications such as stopping smoking can be provided to patients to try and reduce risk.
Patients with one or two HLA-DRB1 SE alleles (vs no allele) are nearly 3 to 5 times as likely to be ACPA seropositive and have erosive disease.4 At high levels, ACPA titres drive the pathophysiology of RA causing significant accelerated bone erosion, which can lead to poor disease prognosis.11 12 13 14 15 16
This is supported by a rheumatology clinician:
"Anti CCP antibodies also activate Osteoclasts resulting in increased erosive disease. The presence of high positive Rheumatoid factor in combination with Anti CCP antibodies further increases the risk of erosions highlighting this particular case as having a poor prognosis without treatment." - Consultant Rheumatologist
Implications on RA
ACPA seropositivity drives highly aggressive, erosive RA.11 12 13 15 16 For patients with RA who have poor prognosis, being initiated and remaining on treatment is critical to prevent disease progression.14 15 16 17

However, the increased risk of serious infection associated with rheumatoid arthritis is well documented with some studies suggesting a greater than 2-fold increased risk of serious infection.18 Therefore, initiating therapies which may expose patients to further infection risk is a major concern for physicians.
Co-morbidities affecting the respiratory tract, such as interstitial lung disease (ILD), further increase the risk of infection for patients with rheumatoid arthritis, providing additional complications.19 20 Find out more about patients with RA-ILD here.
"In patients with Rheumatoid arthritis , anti CCP antibodies in inflamed synovium have been shown to associate with citrullinated antigens to form immune complexes, resulting in progression of the inflammatory process and probably explains why CCP positive patients have a more erosive disease course than sero-negative patients." - Consultant Rheumatologist
What do the guidelines say?
NICE guidelines call for ACPA serostatus testing as soon as possible after diagnosis to facilitate and guide appropriate treatment decisions.21
COVID-19 has highlighted the importance of considering infection risk when making treatment decisions with emergency NICE guidance suggesting that patients with RA should avoid attending face to face consultations wherever possible.22 23 The guidance goes one step further in recommending that patients receiving intravenous biologic therapy be switched to the same treatment in subcutaneous form, and where this is not possible, discussing an alternative subcutaneous treatment.22
Various studies have demonstrated that biologic molecules have different profiles of infection risk.24 25 26 The British Society for Rheumatology biologic DMARD safety guidelines in inflammatory arthritis take account of this by recommending that use of abatacept or etanercept should be considered in patients who are at high risk of infection.27
Despite guideline recommendations, and evidence showing some biologics have a better infection risk and safety profile, in practice this is not acknowledged, with market research demonstrating the first line biologic used most often is the one with the highest risk of infection and mortality.
Implications on clinical practice
Keeping patients out of hospital is a key treatment consideration to minimise infection risk. The importance of this has somewhat been compounded by the Covid-19 pandemic.
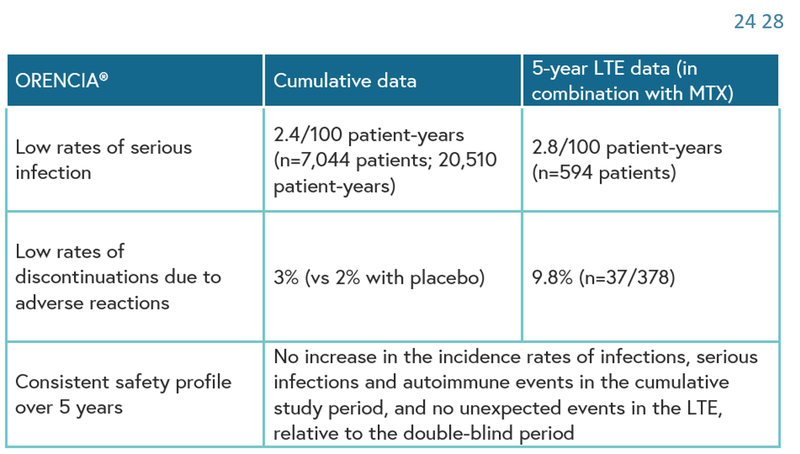
Orencia (abatacept) may be a suitable choice for patients with poor prognosis due to its acceptable long-term safety profile across clinical studies.24 28 Low rates of serious infections and discontinuations due to adverse reactions have been observed in patients treated with Orencia.24 28
In MTX-refractory patients with RA, longterm ABA treatment was well tolerated and provided consistent safety and sustained efficacy, with high patient retention. Radiographic progression continued to be inhibited with ongoing treatment.28 Abatacept has been studied in patients with active rheumatoid arthritis in placebo-controlled clinical trials (2,653 patients with abatacept, 1,485 with placebo).24
Serious infections, including sepsis and pneumonia, have been reported with abatacept. Some of these infections have been fatal. Treatment with ORENCIA should not be initiated in patients with active infections until infections are controlled. Physicians should exercise caution when considering the use of ORENCIA in patients with a history of recurrent infections or underlying conditions which may predispose them to infections. Administration of ORENCIA should be discontinued if a patient develops a serious infection.
The use of abatacept in patients with seropositive rheumatoid arthritis is supported by consultant rheumatologists who stated:
"The good thing about abatacept is the ease of use: No need for complicated monitoring." - Consultant Rheumatologist
Furthermore, Orencia is supported by a Homecare programme enabling use in community settings.